Hereditary Hemochromatosis vs. Wilson Disease
General Features
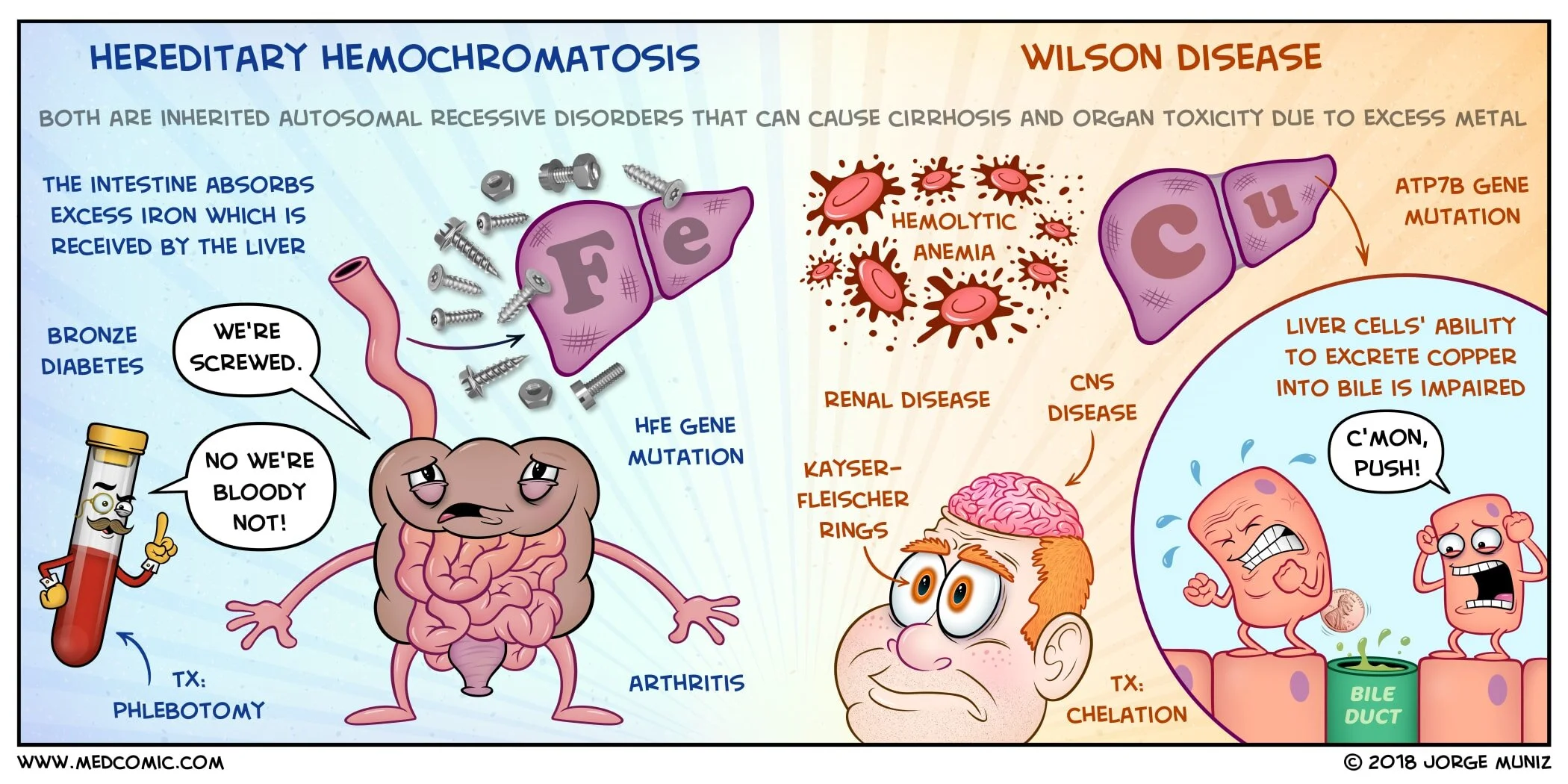
Hereditary hemochromatosis: disorder of iron overload
Accumulation of iron resulting in toxicity of the liver, pancreas, joints, skin, heart, and endocrine organs
Wilson disease (hepatolenticular degeneration): disorder of copper overload
Accumulation of copper resulting in toxicity of the liver, kidneys, brain, eyes, heart, and red blood cells
Both hereditary hemochromatosis and Wilson disease are inherited, autosomal recessive disorders that can cause cirrhosis due to excess metal accumulation
Hereditary hemochromatosis: mutation in the HFE gene
Common mutations: C282Y and H63D
Wilson disease: mutation in the ATP7B gene
The liver is the main organ affected by excess of both metals, but the mechanism of metal accumulation and overload differs
Hereditary hemochromatosis: the liver receives excess iron
The intestinal mucosa absorbs excess amounts of dietary iron which is received passively by the liver
Wilson disease: the liver accumulates excess copper inside liver cells
Liver cells have an impaired ability to excrete copper into bile
There is also impaired binding of copper to ceruloplasmin
Clinical Features and Diagnosis
Patients may be asymptomatic
Hereditary hemochromatosis: hepatic fibrosis or cirrhosis, arthritis, diabetes mellitus, skin pigmentation (“bronze diabetes”), loss of libido/impotence, cardiomyopathy, and other endocrine disorders
Elevated fasting serum transferrin saturation greater than 45-50%, ferritin greater than 300 ng/mL in men and greater than 200 ng/mL in women, and increased iron
HFE gene testing
Liver biopsy may be helpful in determining the degree of fibrosis
Imaging studies such as CT and particularly MRI may detect heavily iron-loaded individuals, but are not reliable methods to make the definitive diagnosis
Wilson disease: cirrhosis, chronic hepatitis, fulminant hepatic failure, neuropsychiatric disorders, Kayser-Fleischer rings, renal disease, hemolytic anemia, cardiomyopathy
Elevated serum copper, low serum ceruloplasmin less than 20 mg/dL (but can be normal), and elevated 24-hour urinary copper greater than 100 μg/day
Liver biopsy should be performed for quantitative measurement of hepatic copper
Treatment
Hereditary hemochromatosis: phlebotomy (weekly or biweekly) until ferritin level is less than 50 ng/mL and the transferrin saturation is less than 50%, followed by life-long maintenance phlebotomies every 2 to 4 months once excess iron stores are removed
Wilson disease: decrease dietary copper, copper-chelating agents such as d-penicillamine or trientine, oral zinc supplementation (interferes with copper absorption in the GI tract), liver transplant for end-stage disease
Family screening for all first-degree relatives (both hereditary hemochromatosis and Wilson disease)